
- Center for Medicare Advocacy Toolkit: How to Obtain an Additional 100 Days of Medicare Coverage in a Skilled Nursing Facility During the COVID Public Health Emergency
- Cobra Notices Revised to Include More Medicare Information
- What’s New in Infection Control Surveys for Nursing Facilities?
- Register Now – Free Educational Webinar Series for 2020-2021
As the Public Health Emergency (PHE) continues and the number of Medicare beneficiaries impacted by the PHE grows, the Center for Medicare Advocacy (the Center) has received an increasing number of requests for guidance on expanded Medicare coverage in skilled nursing facilities (SNFs).
The following are a compilation of self-help materials that include articles written by the Center (citing CMS guidance), detailed CMS instructions to obtain the waiver, and an interpretation of the additional 100 day waiver as adjudicated by a Medicare Administrative Law Judge (ALJ):
- Our July 2020 CMA Alert discussing the Centers for Medicare and Medicaid Services (CMS) detailed guidance about how to obtain up to an additional 100 days of SNF coverage. https://medicareadvocacy.org/cms-clarifies-covid-waivers/
- A June 2020 CMA Alert discussing a case study of the 100 day waiver and a full explanation of when the additional coverage would apply, and when it would not. Here is a link to the article: https://medicareadvocacy.org/covid-19s-impact-on-beneficiary-rights-a-case-study-examining-medicare-coverage-exceeding-100-days-in-a-skilled-nursing-facility/
Traditional Medicare Cases: CMS has issued a Medicare Learning Network (MLN) article that explains exactly how to bill for the 100 days, including necessary coding and language required to be included in the remarks section (COVID100). Without working through the specific billing requirements, CMS states that the claim will not be processed. https://www.cms.gov/files/document/se20011.pdf
Medicare Advantage Plan Cases: A Medicare ALJ decision shared with the Center by a beneficiary details the steps used by the ALJ to award an additional 100 days of coverage, overruling organization determinations and the independent review entity’s denial of the additional days. The redacted decision is at: https://medicareadvocacy.org/wp-content/uploads/2020/09/COVID-19-100-extra-days-in-SNF-OMHA-decision.pdf.
A note of caution about Medicare’s 1135 blanket waivers, providing flexibility under section 1812(f) of the Social Security Act: A PHE waiver that extends SNF benefits by up to 100 days does not appear to afford beneficiaries the same rights as the first 100 days of statutory coverage. In a letter written in response to a congressional inquiry about the issue, CMS noted that the benefit extension under the PHE is at the discretion of the facility. CMS stated, “Our goal with these waivers is to provide flexibility for the wide variety of challenges that SNFs face during the pandemic. In such circumstances, blanket waivers allow facilities to apply provisions without the need to request them from CMS, thereby allowing SNFs to address very local and very specific challenges. If the SNF would like to cite and document…The SNF may choose to exercise that provision of the 1135 blanket SNF waiver…” The redacted CMS letter is at: https://medicareadvocacy.org/wp-content/uploads/2020/09/CMS-redacted-letter-re_-congressional-inquiry-PHE-100-day-waiver.pdf
– top –
Cobra Notices Revised to Include More Medicare Information
As the Center for Medicare Advocacy wrote in our January 2020 CMA Alert, the Chairmen and Ranking Members of the House Ways & Means, Energy & Commerce, and Education & Labor Committees sent a letter that month to the Secretaries of Health and Human Services (HHS) and Department of Labor (DOL) asking the “agencies to address the confusion and financial risks that often confront Americans who are Medicare-eligible and receive coverage under a group health plan subject to the Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA).” See the press release issued by the Energy & Commerce Committee here.
Due to the complex rules surrounding Medicare secondary payment, coordination of benefits, and Part B enrollment, coupled with a lack of adequate information provided to former employees who choose to take COBRA coverage when they are eligible (or near eligibility) for Medicare, such individuals often face “unexpected penalties and unnecessary out-of-pocket expenses” (see, e.g., CMA Alerts the Center wrote in November 2015 about problems surrounding the interaction between COBRA and Medicare: Parts I, II and III).
The Committees called on the federal agencies to “develop a strategy that effectively addresses the issue and to produce informative and clear communications for affected Americans.” The Center for Medicare Advocacy strongly supports this effort.
Updated Model COBRA Notices
In May 2020 the Department of Labor released updated model COBRA notices and Frequently Asked Questions (FAQs) that address Medicare coverage. These documents are available here.
The Medicare-related language in the Model General Notice includes the following (at p. 3):
Can I enroll in Medicare instead of COBRA continuation coverage after my group health plan coverage ends?
In general, if you don’t enroll in Medicare Part A or B when you are first eligible because you are still employed, after the Medicare initial enrollment period, you have an 8-month special enrollment period to sign up for Medicare Part A or B, beginning on the earlier of
- The month after your employment ends; or
- The month after group health plan coverage based on current employment ends.
If you don’t enroll in Medicare and elect COBRA continuation coverage instead, you may have to pay a Part B late enrollment penalty and you may have a gap in coverage if you decide you want Part B later. If you elect COBRA continuation coverage and later enroll in Medicare Part A or B before the COBRA continuation coverage ends, the Plan may terminate your continuation coverage. However, if Medicare Part A or B is effective on or before the date of the COBRA election, COBRA coverage may not be discontinued on account of Medicare entitlement, even if you enroll in the other part of Medicare after the date of the election of COBRA coverage.
If you are enrolled in both COBRA continuation coverage and Medicare, Medicare will generally pay first (primary payer) and COBRA continuation coverage will pay second. Certain plans may pay as if secondary to Medicare, even if you are not enrolled in Medicare.
For more information visit https://www.medicare.gov/medicare-and-you.
The Medicare-related language in the FAQ document includes the following:
Q2: I didn’t enroll in Medicare when I first became eligible because I was still employed, but I recently lost my job. Can I enroll in Medicare now after my group health plan coverage ends?
Yes, and there may be advantages to enrolling in Medicare before, or instead of, electing COBRA. In general, if you don’t enroll in Medicare Part A or B when you are first eligible because you are still employed, after the Medicare initial enrollment period, you have an 8-month special enrollment period to sign up for Medicare Part A or B, beginning on the earlier of
- The month after your employment ends; or
- The month after group health plan coverage based on current employment ends.
If you don’t enroll in Medicare and elect COBRA continuation coverage instead, you may have to pay a Part B late enrollment penalty and you may have a gap in coverage if you decide you want Part B later. If you elect COBRA continuation coverage and later enroll in Medicare Part A or B before the COBRA continuation coverage ends, the Plan may terminate your continuation coverage. However, if Medicare Part A or B is effective on or before the date of the COBRA election, COBRA coverage may not be discontinued on account of Medicare entitlement, even if you enroll in the other part of Medicare after the date of the election of COBRA coverage
Q3: What health coverage pays first if I’m enrolled in both Medicare and COBRA?
If you are enrolled in both COBRA continuation coverage and Medicare, Medicare will generally pay first (primary payer) and COBRA continuation coverage will pay second. Certain plans may pay as if secondary to Medicare, even if you are not enrolled in Medicare.
Conclusion
While the new Medicare-related language in the model COBRA notices is not comprehensive (e.g., it does not address potential impacts on spousal coverage, and how COBRA might work differently for individuals with ESRD), and does not include a strong enough warning about the dangers of foregoing Part B coverage and retaining COBRA coverage, it will hopefully help some people avoid the pitfalls of Part B enrollment problems associated with COBRA coverage.
– top –
What’s New in Infection Control Surveys for Nursing Facilities?
The Centers for Medicare & Medicaid Services (CMS) has revised the focused infection control survey protocol.[1] Now, for the first time, CMS requires surveyors to review the care actually provided to a sample of residents (and among a sample of staff). This important change, supported by the Center for Medicare Advocacy (Center), may result in the citation of more infection control deficiencies than prior focused infection control surveys, which appeared to be limited in scope, short in duration (one surveyor conducted several surveys in one day), and more focused on paperwork compliance than on observing whether staff providing care to residents correctly and consistently followed longstanding infection control practices.
Accurate citing of deficiencies is a key component of the oversight system for nursing facilities. If deficiencies are not cited, facilities will operate under the assumption they have no problems in their infection control practices and they will not make any changes or corrections.
The Center for Medicare Advocacy has contended that the limited number of deficiencies that have been cited during the COVID-19 pandemic is not plausible when so many residents and staff are dying from the coronavirus. This is further unlikely when, as reported by the Government Accountability Office in May 2020, infection control deficiencies before the pandemic were “widespread” and “persistent.”[2]
On August 14, 2020, CMS reported that it had cited more than 180 facilities with immediate jeopardy infection control deficiencies (triple the rate in 2019) and imposed civil money penalties of nearly $10 million, averaging $55,000 for each facility.[3] As we have reported,[4] CMS told residents’ advocates in an August 19, 2020 call that information about these surveys, to date, was reported only on an internal CMS database; these surveys had not been publicly reported. As described below, publicly reported infection control data, released by CMS on August 26, continue to show many fewer immediate jeopardy infection control deficiencies than CMS reports having cited – 48, compared to nearly 180.
However, news reports indicate more deficiencies and penalties than CMS publicly reports. For example, on September 2, 2020, the Baltimore Sun reported that state inspection reports show infection control deficiencies were cited at 64 Maryland nursing facilities, with ten facilities facing fines ranging from $70,000 to $380,000.[5] The Collingswood Rehabilitation and Healthcare Center was fined $275,000 in June. CMS’s cumulative data release of August 26 reports only a March 4 survey at Collingswood that did not cite an infection control deficiency; the release does not show any survey at Collingswood citing an infection control deficiency.
CMS’s August 26 Cumulative Data Release
On August 26, 2020, CMS made public the fourth cumulative release of 25,593 targeted infection control surveys, covering the period March 4 through July 31. The surveys cited 556 infection prevention and control deficiencies in 539 facilities (524 facilities were cited with one deficiency, 13 facilities were cited with two deficiencies, two facilities were cited with three deficiencies).
Of the 556 infection control deficiencies, 48 deficiencies (8.6%) were cited at the immediate jeopardy level.
Although all four releases of infection control surveys and deficiencies show that less than 3% of focused infection control surveys cited deficiencies, an increasing percentage of these deficiencies has been classified as immediate jeopardy.
| Date of CMS Release | Number of Surveys | Number (%) of infection control deficiencies cited | Number (%) of infection control deficiencies classified as immediate jeopardy |
| June 4 | 5,724 | 163 (2.8%) | 1 (1.0%) |
| June 24 | 9,899 | 262 (2.6%) | 4 (1.5%) |
| July 29 | 16,987 | 347 (2.0%) | 22 (6.6%) |
| August 26 | 25,593 | 556 (2.2%) | 48 (8.6%) |
The surveys released in August also show that:
- The scope of deficiencies has shifted. While the first three cumulative releases showed that the largest category of deficiencies was cited as “few,” the fourth cumulative release shows that “some” is now the largest category with respect to scope of deficiencies.
- Most deficiencies (503 of 556 deficiencies, 90.5%) are cited as minimal harm or potential for actual harm (levels D, E, and F), also known as “no harm” deficiencies.
- “No harm” deficiencies (levels D, E, and F) were predominant in all four cumulative releases of infection control surveys.
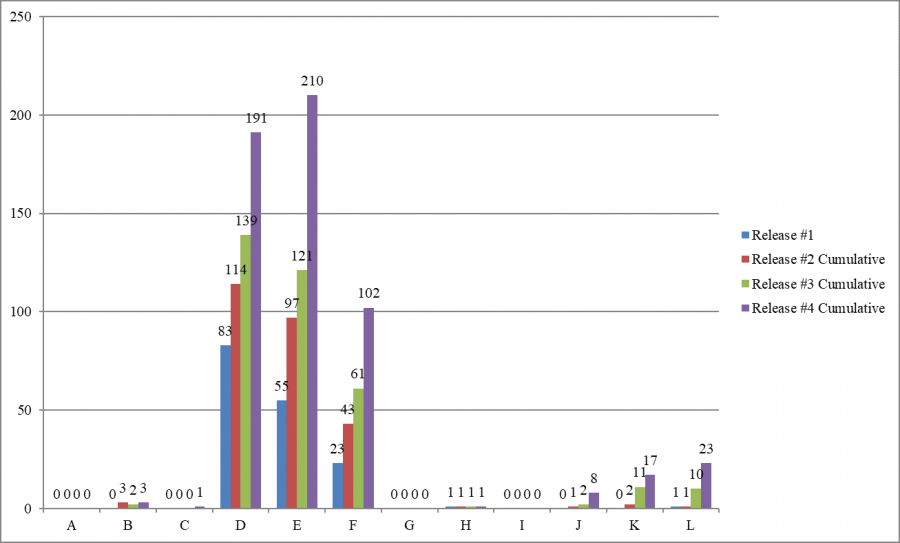
- As in previous releases, Texas cited more infection control deficiencies than any other state – 120 of 556 deficiencies (21.6% of the infection control deficiencies cited nationwide).
Conclusion
The revised survey protocol may lead to a more accurate evaluation of facilities’ failures to comply with infection control requirements.
Although an increasing proportion of the deficiencies is classified as immediate jeopardy, the 48 immediate jeopardy infection control deficiencies publicly reported in August are still far fewer than the nearly 180 number claimed by CMS.
- To read the full report, please go to: https://medicareadvocacy.org/wp-content/uploads/2020/09/Special-Report-Whats-New-In-Infection-Control.pdf
__________________
[1] CMS, “Interim Final Rule (IFC), CMS-3401-IFC, Additional Policy and Regulatory Revisions in Response to the COVID-19 Public Health Emergency related to Long-Term Care (LTC) Facility Testing Requirements and Revised COVID-19 Focused Survey Tool,” QSO-20-38-NH (Aug. 26, 2020), https://www.cms.gov/files/document/qso-20-38-nh.pdf.
[2] GAO, “Infection Control Deficiencies Were Widespread and Persistent in Nursing Homes Prior to COVID-19 Pandemic,” GAO-20-576R (May 20, 2020), https://www.gao.gov/assets/710/707069.pdf. The report is discussed in CMA, “GAO on Infection Control Deficiencies in Nursing Facilities Before Covid-19 Pandemic: ‘Widespread,’ ‘Persistent,’ ‘Ignored’” (CMA Alert, May 21, 2020), https://medicareadvocacy.org/gao-widespread-snf-deficiencies/.
[3] CMS, “Trump Administration Has Issued More Than $15 Million in Fines to Nursing Homes During COVID-19 Pandemic” (Press Release, Aug. 14, 2020), https://www.cms.gov/newsroom/press-releases/trump-administration-has-issued-more-15-million-fines-nursing-homes-during-covid-19-pandemic.
[4] CMA, “Responding to CMS Announcement on Nursing Home Enforcement – Infection Control Deficiencies in Nursing Facilities: QCOR Data” (CMA Alert, Aug. 20, 2020), https://medicareadvocacy.org/responding-to-cms-announcement-on-nursing-home-enforcement-infection-control-deficiencies-in-nursing-facilities-qcor-data/.
[5] Meredith Cohn, “Dozens of Maryland nursing homes found with deficient infection control during coronavirus pandemic,” Baltimore Sun (Sep. 2, 2020), https://www.baltimoresun.com/coronavirus/bs-hs-nursing-home-covid-inspections-20200902-ajvxfl76lba6xn6u7bitx7crpm-story.html.
– top –
Register Now – Free Educational Webinar Series for 2020-2021
Please consider a donation to help us continue to provide these programs at no charge.
This presentation will explore the role Medicare does, and could, play in supporting older and disabled beneficiaries and their caregivers.
Wednesday, September 9, 2020 2:00 PM – 3:00 PM EDT
Presenters: Center for Medicare Advocacy Executive Director Judy Stein, Associate Director David Lipschutz
Register at: https://attendee.gotowebinar.com/register/3946073973903728656
Skilled Nursing Facility Staffing
The Center for Medicare Advocacy has been examining the broad variety of approaches to nurse staffing in nursing homes, and their effectiveness, or lack of effectiveness, in achieving improved staffing levels and competencies. This webinar will discuss some of our findings.
Wednesday September 30,2020 2:00 PM – 3:00 PM EDT
Presenters: Senior Policy Attorney Toby Edelman, Guest
Register at: https://attendee.gotowebinar.com/register/871456832595656976
Medicare Enrollment Issues for 2021
This webinar will discuss the 2020 Annual Coordinated Election Period (ACEP), including outreach and education materials issued by the Medicare program, Medicare Plan Finder updates, common enrollment pitfalls, options when you miss your Initial Enrollment Period, and other considerations for Medicare beneficiaries and those who assist them. Policy changes, potential helpful legislation, and other updates for 2021 will also be discussed, including Medicare Advantage network adequacy and other changes made by final regulations.
Wednesday, October 14, 2020 2:00 PM – 3:00 PM EDT
Presenters: Center for Medicare Advocacy Associate Director David Lipschutz, Sue Greeno, Guest
Register at: https://attendee.gotowebinar.com/register/535147011985794315
Skilled Nursing Facility Update
The webinar will provide an overview of Nursing Home Quality of Care & Quality of Life Standards from a consumer perspective.
Wednesday, December 2, 2020 2:00 PM – 3:00 PM EST
Presenters: Center for Medicare Advocacy Senior Policy Attorney Toby Edelman, Guest
Register at: https://attendee.gotowebinar.com/register/536143169520642059
Medicare & Health Care Updates
This presentation will examine and try to make sense of what’s happening in the Medicare and related health care world, including impacts of COVID-19, from the perspective of beneficiary advocates.
Wednesday, February 3, 2021 2:00 PM – 3:00 PM EST
Presenters: Center for Medicare Advocacy Senior Policy Attorney David Lipschutz, Kata Kertesz, Guests
Register at: https://attendee.gotowebinar.com/register/836653991043094283
This presentation will provide a summary and update of Medicare home health coverage, care, and payment issues. The webinar will focus on the opportunities and challenges facing beneficiaries with longer term and debilitating conditions who need care at home. Practical tips and advocacy guidance will be included.
Wednesday, March 24, 2021 2:00 PM – 3:00 PM EST
Presenters: Center for Medicare Advocacy Executive Director, Attorney Judith Stein, and Associate Director, Attorney Kathy Holt
Register at: https://attendee.gotowebinar.com/register/2614663249203451147
Bonus Webinar – Topic TBD Based on Current Events
Wednesday, May 19, 2021 2:00 PM – 3:00 PM EST
Presenters: TBD
Register at: https://attendee.gotowebinar.com/register/6162491503408897803
– top –