
- Medicare Open Enrollment Starts October 15
- Nursing Facilities and Covid-19 – It’s Not Inevitable
- AHRQ Launches National Nursing Home COVID Action Network Training Program
- Special Report: CMS Releases Fifth Cumulative List of Focused Infection Control Surveys
- State Administrative Law Judge Largely Clears Lifecare Center of Kirkland, First Nursing Home in Country with Covid-19 Outbreak
- Elder Justice Newsletter – Vol 3, Issue 2 Now Available
Medicare Open Enrollment Starts October 15
The Annual Election Period (AEP) – the period during which individuals with Medicare can make coverage elections regarding Medicare Advantage (MA) and Part D plans for the following year – will start October 15th and last until December 7th. This period is sometimes referred to as the Open Enrollment Period (OEP).
For more information on Open Enrollment join us next Wednesday for our free webinar:
Medicare Enrollment Issues for 2021
October 14, 2020 at 2:00 EDT
This webinar will discuss the 2020 Annual Coordinated Election Period (ACEP), including outreach and education materials issued by the Medicare program, Medicare Plan Finder updates, common enrollment pitfalls, options when you miss your Initial Enrollment Period, and other considerations for Medicare beneficiaries and those who assist them. Policy changes, potential helpful legislation, and other updates for 2021 will also be discussed, including Medicare Advantage network adequacy and other changes made by final regulations.
- Register now at: https://medicareadvocacy.org/webinars/
– top –
Nursing Facilities and Covid-19 – It’s Not Inevitable
The nursing home industry claims that outbreaks of COVID-19 in nursing facilities are largely the result of geography and that once coronavirus gets into a building, it inevitably spreads throughout the facility. Increasing evidence documents that the industry is wrong on both counts.
In a Message to his members, the American Health Care Association’s President and CEO Mark Parkinson wrote in June, in an explanation of How Did We Get Here?:
It wasn’t a matter of bad operators getting COVID-19 and good operators not getting it. The facts indicate that your Five-Star rating, profit vs. not for profit status, or prior deficiency history are not predictors of whether COVID-19 gets in your buildings. The most important factor in determining whether COVID-19 ends up in a building is the surrounding community of where the building is located. If you are located in New York, you likely ended up with COVID-19 in your building. If you are located in the rural Midwest, you are less likely to have COVID-19 in your building. It depends on the outbreak in the surrounding community, which impacts the number of carriers without symptoms.[1]
Geography is not the sole determinant of COVID-19. Facilities providing higher quality of care are less likely to experience COVID-19 outbreaks. An analysis of West Virginia nursing facilities by the Centers for Disease Control and Prevention (CDC) finds that “the odds of a COVID-19 outbreak were 87% lower among 2- to 3-star-rated facilities and 94% lower among 4- to 5-star-rated facilities.”[2]
Individual nursing facilities also give lie to the “geography is destiny” myth. An article in the Washington Post describes the Maryland Baptist Aged Home, the oldest black-owned nursing facility in the state serving primarily low-income Black and Latinx adults. As of the July 24 article, the Baltimore facility had remained entirely COVID-free during the pandemic, even as 338 people in its zip code, and more than 13,000 residents and staff in Maryland, had been infected.[3] The Maryland Baptist Aged Home, with 29 residents, has had a full-time infection control nurse on staff for 10 years and has not been cited with an infection control deficiency in four years.
Similarly, containment of COVID-19 is more successful in some facilities than in others. As the Center for Medicare Advocacy reported in August,[4] multiple studies find that nursing facilities with higher nurse staffing levels are more successful in containing COVID-19 than facilities with lower staffing levels. For example, an analysis of all 215 Connecticut nursing facilities with confirmed COVID-19 cases and deaths as of April 16, 2020 finds that every 20 minutes per resident day of increased staffing by registered nurses was associated with 22% fewer confirmed cases of COVID-19 and 26% fewer COVID-19 deaths.[5]
An analysis of nursing facilities in New York State also found that, compared to facilities without labor unions, facilities with unions had a 30% lower mortality rate from COVID-19 and a 42% “relative decrease in COVID-19 infection rates” among residents.[6] Facilities with unions were located in counties with higher rates of COVID-19 than facilities without unions, countering the industry argument that zip code determines COVID-19 infection rates.
Conclusion
The Center for Medicare Advocacy does not contend that the location of a facility has absolutely no effect on COVID-19 infection rates in nursing facilities. However, it is not the sole factor. While the Kaiser Family Foundation reported in July that hotspots of COVID-19 witnessed an increased in COVID-19 in their nursing facilities, its data actually showed that the increase in COVID-19 in facilities was considerably lower than the COVID-19 increase in the state.[7] In Florida, for example, COVID-19 increased by 96% in the state between June 24 and July 9, but COVID-19 increased by 51% in nursing facilities for the same 10-day period. In the other hotspot state, Texas, COVID-19 increased by 89% in the state and by 47% in nursing facilities during the same period.[8]
We cannot allow to go unchecked the nursing home industry’s argument that COVID-19 in the community always means COVID-19 in facilities and that facilities are without responsibility for containing the virus. High staffing levels, good infection control practices, and sufficient testing and personal protective equipment are all critical factors determining whether COVID-19 gets into nursing facilities and whether it spreads.
____________________
[1] American Health Care Association, “We Won’t Back Down” (Jun. 2020), https://files.constantcontact.com/64f0b60b701/f86b03a3-a859-4098-b6d0-3866c56672d5.pdf, discussed in “American Health Care Association’s CEO Issues Message to Members: ‘We Won’t Back Down,’” (CMA Alert, Jul. 16, 2020), https://medicareadvocacy.org/american-health-care-associations-ceo-issues-message-to-members-we-wont-back-down/. Parkinson cited David Grabowski, Professor of Health Policy, Harvard Medical School, as a key researcher finding that COVID-19 is a function of geography. At a presentation on October 6, 2020 at a webinar sponsored by the Alliance for Health Care Reform, Professor Grabowski reiterated the claim that geography is key. Addressing which nursing homes have COVID, he said “Where you are, not who you are.” Later, in response to a question, he acknowledged that the number of staff can be a way to prevent a huge outbreak.
[2] David P. Bui, et al, “Association Between CMS Quality Ratings and COVID-19 Outbreaks in Nursing Homes – West Virginia, March 17-June 11, 2020,” CDC Morbidity and Mortality Report (Sep. 18, 2020), MMWR Morb Mortal Wkly Rep 2020; 69:1300-1304, https://www.cdc.gov/mmwr/volumes/69/wr/pdfs/mm6937a5-H.pdf.
[3] Rebecca Tan, “In Baltimore, a struggling, black-owned nursing home keeps covid-19 at bay,” Washington Post (Jul. 24, 2020), https://www.washingtonpost.com/local/baltimore-nursing-home-covid-free/2020/07/23/31bddade-c78a-11ea-b037-f9711f89ee46_story.html.
[4] See CMA, “Studies Find Higher Nurse Staffing Levels in Nursing Facilities Are Correlated With Better Containment of COVID-19” (CMA Alert, Aug. , 2020).
[5] Yue Li, H Temkin-Greener, S Gao, X. Cai, “COVID-19 infections and deaths among Connecticut nursing home residents: facility correlates,” Journal of American Geriatrics Society (2020), https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgs.16689.
[6] Adam Dean, Atheendar Verkataramani, and Simeon Kimmel, “Mortality Rates From COVID-19 Are Lower In Unionized Nursing Homes,” Health Affairs (published Sep. 10, 2020), https://www.healthaffairs.org/doi/10.1377/hlthaff.2020.01011, discussed in CMA, “Study Finds Lower Mortality Rates in Unionized New York State Nursing Facilities” (CMA Alert, Sep. 17, 2020), https://medicareadvocacy.org/study-finds-lower-mortality-rates-in-unionized-new-york-state-nursing-facilities/.
[7] Priya Chidambaram, “Rising Cases in Long-term Care Facilities Are Cause for Concern,” Kaiser Family Foundation Data Note (Jul. 21, 2020), https://www.kff.org/coronavirus-covid-19/issue-brief/rising-cases-in-long-term-care-facilities-are-cause-for-concern/.
[8] Id. Table 1.
– top –
AHRQ Launches National Nursing Home COVID Action Network Training Program
About 40% of all COVID-19 related deaths in the United States, according to The New York Times, are linked to nursing homes. To help combat these startling statistics, the Centers for Disease Control and Prevention (CDC) states that “a strong infection prevention and control program is critical to protect both residents and healthcare personnel.”
The Agency for Healthcare Research and Quality (AHRQ) is launching the National Nursing Home COVID Action Network which will offer free training and mentorship to nursing homes around the nation with the goal of increasing the implementation of evidence-based infection prevention and safety practices to protect residents and staff. AHRQ is partnering with the University of New Mexico’s ECHO Institute and the Institute for Health Care Improvement (IHI) to provide these trainings. This program was created under an AHRQ contract which is part of the nearly $5 billion Provider Relief Fund authorized by the CARES Act.
The National Nursing Home COVID Action Network joins a series of other programs already in place. As reported in CMA’s COVID-19: Advocate’s Guide, in May the Centers for Medicare & Medicaid Services (CMS) and the Quality Improvement Organization (QIO) Program launched an eight-week national nursing home training series on infection prevention for nursing facilities. Additionally, CMS and the CDC have developed an on-demand “Nursing Home COVID-19 Training” offering to supplement existing training with education on cohorting strategies, as well as telehealth use.
– top –
Special Report: CMS Releases Fifth Cumulative List of Focused Infection Control Surveys
On September 30, 2020, the Centers for Medicare & Medicaid Services (CMS) released its fifth cumulative report on focused infection control surveys in nursing facilities. Like previous reports, the fifth report shows that comparatively few facilities are cited with deficiencies and that most deficiencies are called “no harm.”
On August 14, 2020, CMS reported that it had cited more than 180 facilities with immediate jeopardy infection control deficiencies (triple the rate in 2019) and imposed civil money penalties of nearly $10 million, averaging $55,000 for each facility.[1] As reported by the Center,[2] CMS told residents’ advocates in an August 19 call that information about these surveys, to date, was reported only on an internal CMS database. All the survey reports identified by CMS nearly two months ago have still not been publicly reported. As described below, publicly reported infection control data, released by CMS on September 30 (and covering the period through August 31), continue to show many fewer immediate jeopardy infection control deficiencies than CMS reports having cited in mid-August – 75, compared to 180.
News reports continue to indicate that more deficiencies have been cited and more penalties have been imposed than CMS publicly reports. For example, ABC News reported that since March 1, 2020, New York State has cited infection control deficiencies at 62 nursing facilities, about one in ten facilities in the state, and determined that six violations placed residents in immediate jeopardy. ABC News also reported that the state imposed fines totaling $328,000 at 23 facilities for infection control deficiencies. The largest fine, $50,000, was imposed at Humboldt House Rehab and Nursing Center in Buffalo, where residents with and without COVID-19 were commingled.[3]
CMS’s September 30 Cumulative Data Release
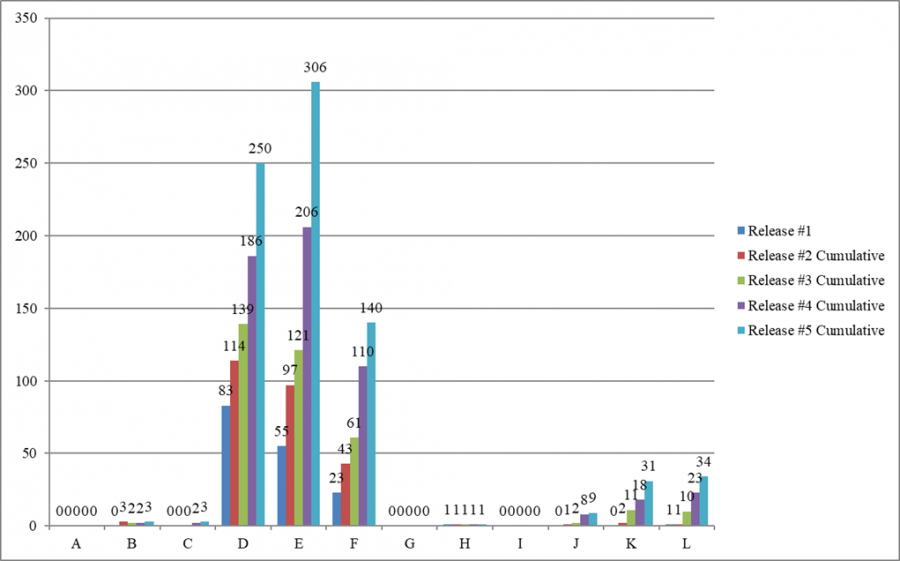
On September 30, 2020, CMS made public the fifth cumulative release of 32,681 targeted infection control surveys, covering the period March 4 through August 31. The surveys cited 777 infection prevention and control deficiencies in 742 facilities (711 facilities were cited with one deficiency, 27 facilities were cited with two deficiencies, and four facilities were cited with three deficiencies).
Of the 777 infection control deficiencies, 75 deficiencies (9.7%) were cited at the immediate jeopardy level. Although all five releases of infection control surveys and deficiencies show that less than 3% of focused infection control surveys cited deficiencies, an increasing percentage of these deficiencies has been classified as immediate jeopardy.
| Date of CMS release | Number of surveys | Number (%) of infection control deficiencies cited | Number (%) of infection control deficiencies classified as immediate jeopardy |
| June 4 | 5,724 | 163 (2.8%) | 1 (1.0%) |
| June 24 | 9,899 | 262 (2.6%) | 4 (1.5%) |
| July 29 | 16,987 | 347 (2.0%) | 22 (6.6%) |
| August 26 | 25,593 | 556 (2.2%) | 48 (8.6%) |
| September 30 | 32,681 | 777 (2.4%) | 75 (9.7%) |
However, “no harm” deficiencies (levels D, E, and F) have been predominant in all four cumulative releases of infection control surveys.
To read the full report, please go to: https://medicareadvocacy.org/wp-content/uploads/2020/10/Special-Report-5th-Cumulative-Infection-Control-Surveys-PDF-00436350xC6348.pdf
____________________
[1] CMS, “Trump Administration Has Issued More Than $15 Million in Fines to Nursing Homes During COVID-19 Pandemic” (Press Release, Aug. 14, 2020), https://www.cms.gov/newsroom/press-releases/trump-administration-has-issued-more-15-million-fines-nursing-homes-during-covid-19-pandemic.
[2] CMA, “Responding to CMS Announcement on Nursing Home Enforcement – Infection Control Deficiencies in Nursing Facilities: QCOR Data” (CMA Alert, Aug. 20, 2020), https://medicareadvocacy.org/responding-to-cms-announcement-on-nursing-home-enforcement-infection-control-deficiencies-in-nursing-facilities-qcor-data/.
[3] Marina Villeneuve, Associated Press, “Inspections found nursing home lapses as COVID-19 raged,” ABC News (Sep. 24, 2020), https://abcnews.go.com/Health/wireStory/inspections-found-nursing-home-lapses-covid-19-raged-73223780.
– top –
Life Care Center of Kirkland (LCCK) was the first nursing facility in the United States where the coronavirus pandemic broke out. More than 30 residents at the Seattle nursing facility died of COVID-19 in March 2020. Between March 6 and 16, two federal surveyors conducted an on-site inspection at the facility, with assistance by off-site state surveyors. The state cited numerous federal and state deficiencies and imposed stop placement and conditions on the facility’s license. The facility appealed. State Administrative Law Judge (ALJ) Matt Perkins held a hearing June 15-18, 2020. Fourteen witnesses testified, including three witnesses who testified for the state. The facility’s 11 witnesses included two physician expert witnesses; the state did not call any expert witnesses.
In a decision dated September 22, Judge Perkins found:
the Department provided relatively little evidence that the facility actually failed to meet any expected standard of care or failed to follow public health guidelines. In a general sense, the Department seems to have reasoned that, because the outcome was tragic, LCCK must have failed to adequately care for their patients; this idea is based on hindsight.
Decision 35. The ALJ concludes that the facility did not violate state rules on physician services, infection control, general administration, medical director, clinical records, quality assessment and assurance, and quality of care, as alleged by the state, although it violated some requirements. Id. 35-42. He rules that the Department abused its discretion by issuing the stop placement order, but acted within its discretion when it imposed conditions on the facility’s license.
The Centers for Medicare & Medicaid Services cited deficiencies and imposed $611,325 in civil money penalties. A federal administrative appeal of the deficiencies and penalties is scheduled for April 2021.
– top –
Elder Justice Newsletter – Vol 3, Issue 2 Now Available
Elder Justice: What “No Harm” Really Means for Residents is a newsletter published by the Center for Medicare Advocacy and the Long Term Care Community Coalition. The purpose of the newsletter is to provide residents, families, friends, and advocates information on what exactly a “no harm” deficiency is and what it means for nursing home residents. Our latest issue has real stories from nursing homes in New York, Florida, Michigan, and California.
- Read the latest issue at: https://medicareadvocacy.org/wp-content/uploads/2020/10/Elder-Justice-Vol.-3-Issue-2.pdf
– top –