
- House Briefing on Covid and Nursing Homes Highlights Longstanding Problems in Staffing and Infection Control; Committee Launches Investigation of CMS and Five Nursing Home Chains
- Special Report – Nursing Homes Cited with Infection Control Deficiencies During the Pandemic: Poor Results In Health Inspections, Low Staffing Levels
- Administration Issues Final Rule Undermining Non-Discrimination Protections, Days Later Supreme Court Renders Landmark Decision Prohibiting Workplace Discrimination Based on Sexual Orientation and Gender Identity
- COVID-19: An Advocates Guide to Beneficiary Related Medicare Changes – Updated June 16, 2020
- COVID-19: Advocating for Nursing Home Residents – A webinar series
“The Devastating Impact of the Coronavirus Crisis in America’s Nursing Homes,”[1] a June 11 briefing by the Select Committee on COVID of the House Committee on Oversight and Reform, identified nursing homes’ longstanding problems in staffing levels and infection control, as well as the failure of the federal government to take a strong leadership position in confronting the coronavirus pandemic. Based on the Briefing,[2] the Committee on June 16 launched an investigation into the Centers for Medicare & Medicaid Services’s lax oversight of the pandemic and the Trump Administration’s failure to provide testing, supplies, and personal protective equipment to nursing facilities.[3] Chairman Clyburn said, “‘Deregulation and lax enforcement of infection control violations by CMS – both before and during the pandemic – may have contributed to the spread of the virus.’”
The Committee also sent letters to five for-profit nursing home chains (Genesis HealthCare, Life Care Centers of America, Ensign Group, SavaSenior Care, and Consulate Health Care) that provide care to more than 80,000 residents in 40 states and where hundreds of residents have died. The letters seek information about “coronavirus cases and deaths, testing, personal protective equipment, staffing levels and pay, legal violations, and efforts to prevent further infections” as well as information about “the use of federal funds by nursing homes during the pandemic.”
Five witnesses testified at the Committee’s June 11 Briefing: Alison Lolley, daughter of a Louisiana nursing home resident who died of COVID-19 in April; Chris Brown, a certified nursing assistant (CNA) at a Chicago nursing facility; Eric Carlson, Directing Attorney, Justice in Aging; Phil Kerpen, President, American Commitment; and David Grabowski, Professor of Health Care Policy, Harvard Medical School.
The two witnesses closest to day-to-day activities in nursing facilities – Ms. Lolley and Mr. Brown – testified that low staffing levels were a problem even before the pandemic. Ms. Lolley described her mother’s disheveled appearance and statements that she had not been fed, following the March ban on visitors. Mr. Brown, a CNA for 10 years, testified that facilities were and remain understaffed, temporary workers do not have sufficient training or skills to provide necessary care to residents, and facilities continue to lack sufficient tests (he has still not yet been tested for COVID-19) and personal protective equipment (PPE).
The witnesses also generally agreed that the federal government needs to take a leading role in ensuring adequate tests and PPE, but had not done so. A third overriding concern, voiced strongly by Dr. Grabowski, was that data on COVID-19 are inadequate. CMS has required nursing facilities to report COVID-19 deaths and problems since May 8,[4] not since the beginning of the pandemic. “Good public health,” he said, “requires good data.”
_____________
[1] https://oversight.house.gov/legislation/briefings/select-subcommittee-briefing-on-the-devastating-impact-of-the-coronavirus.
[2] The Committee issued a Press Release on June 12, describing key concerns raised by the Briefing. “Select Committee Briefing Confirms Urgent Need for Federal Action to Protect Nursing Homes from Coronavirus” (Press Release, Jun. 12, 2020), https://oversight.house.gov/news/press-releases/select-committee-briefing-confirms-urgent-need-for-federal-action-to-protect.
[3] Select Subcommittee on the Coronavirus Crisis, “Clyburn Launches Sweeping Investigation into Widespread Coronavirus Deaths in Nursing Homes” (Press Release, Jun. 16, 2020), https://coronavirus.house.gov/news/press-releases/clyburn-launches-sweeping-investigation-widespread-coronavirus-deaths-nursing.
[4] Interim final rule, CMS, “Medicare and Medicaid Programs, Basic Health Program, and Exchanges: Additional Policy and Regulatory Revisions in Response to the COVID-19 Public Health Emergency and Delay of Certain Reporting Requirements for the Skilled Nursing Facility Quality Reporting Program,” CMS-5531-IFC, 85 Fed. Reg. 27550 (May 8, 2020), https://www.govinfo.gov/content/pkg/FR-2020-05-08/pdf/2020-09608.pdf.
– top –
Since March 2020, the Centers for Medicare & Medicaid Services (CMS) has limited surveys to two types: targeted infection control surveys and complaints and facility-reported incidents that states triage as immediate jeopardy. The Center for Medicare Advocacy analyzed the infection control surveys released by CMS on June 4, 2020 and found that less than 3% of 5724 infection control surveys resulted in infection control deficiencies; 163 infection control deficiencies were cited at 162 nursing facilities.[1]
The Center has now analyzed the information on Nursing Home Compare for the 160 facilities that were cited with infection control deficiencies.[2] By various measures, these facilities provide poor quality care. Facilities cited with infection control deficiencies had low star ratings, particularly in health surveys, and were more likely to be for-profit facilities. More than 40 percent of the facilities had remedies imposed (civil money penalties) for prior deficiencies and ten facilities were Special Focus Facilities or candidates for the SFF program.
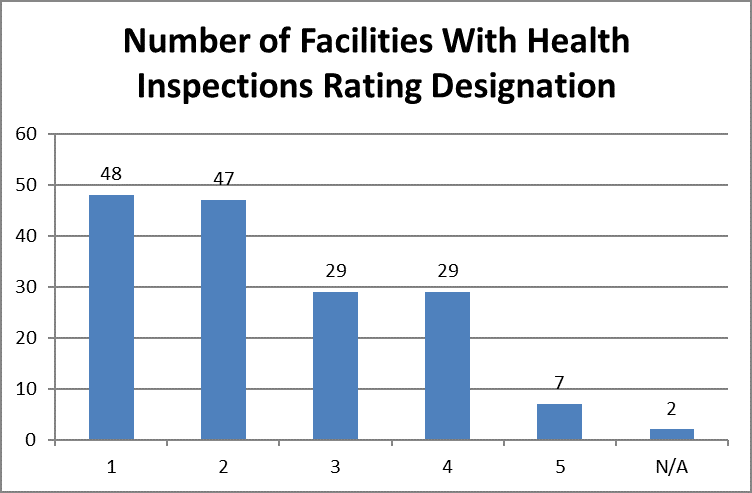
Health Inspections
For example, as shown below, facilities with poorer survey results were more likely to be cited with an infection control deficiency. Of the 160 facilities cited with an infection control deficiency, 95 facilities (59.4 percent) had one or two stars in health inspection surveys. Only 36 facilities with four or five stars (22.5 percent) in health inspection surveys were cited with an infection control deficiency.
- To read the full report, please go to: https://medicareadvocacy.org/wp-content/uploads/2020/06/Coronavirus-Report-Infection-Control-Deficiencies-NHC.pdf
________________
[1] Center for Medicare Advocacy, “Infection Control Surveys at Nursing Facilities: CMS Data Are Not Plausible” (Report, Jun.11, 2020), https://medicareadvocacy.org/wp-content/uploads/2020/06/Infection-Control-Surveys-Report.pdf.
[2] The 163 deficiencies were cited in 162 distinct nursing facilities. Two other facilities are excluded from this analysis of star rating because they were Special Focus Facilities (SFF); CMS does not report star ratings for SFFs.
– top –
Over the last week, the country has taken both a step backward and a step forward with respect to protections against discrimination: One a final rule by the Trump Administration rolling back critical non-discrimination provisions in health care, including for the LGBTQ community; the other, a landmark Supreme Court decision affirming protections against employment discrimination based on sexual orientation and gender identity. Efforts are now underway to reconcile the two. The Supreme Court’s holding, that sex discrimination encompasses discrimination based on gender identity or sexual orientation, should prevail and should be applied in the health care context.
The ACA’s Section 1557: Non-Discrimination
The Health Care Rights Law (Section 1557 of the Affordable Care Act [ACA]), prohibits discrimination in health care on the basis of race, color, national origin, sex, age, and disability. After an extensive process to develop implementing regulations during the Obama Administration, released in 2016, the Trump Administration reopened the regulations for the purpose of rolling back such protections. The Center for Medicare Advocacy joined many other organizations in opposing the Administration’s efforts to limit the law’s protections for individuals who have limited English proficiency, LGBTQ persons, and persons with disabilities and chronic conditions, among others.
On June 12, 2020, the Trump Administration’s Department of Health and Human Services’ (DHSS) Office of Civil Rights (OCR) issued a final rule on Section 1557, which, among other things, removed protections for sex discrimination that is based on gender identity. According to a detailed analysis of the final rule by Katie Keith, published in Health Affairs, “The final rule eliminates major parts of the 2016 regulation and tries to make significant changes to the scope of Section 1557. The final rule entirely eliminates:
- The definitions section of the current rule (thereby eliminating definitions of key terms such as “covered entity” and “on the basis of sex”);
- Specific nondiscrimination protections based on sex, gender identity, and association;
- Major language access requirements (such as a requirement that covered entities include translated taglines on notices and other significant communications to consumers);
- Notice requirements that require covered entities to post information about Section 1557 and nondiscrimination at their locations and on their websites;
- Requirements to have a compliance coordinator and a written grievance procedure to handle complaints about alleged violations of Section 1557; and
- Various enforcement-related provisions (such as protections against intimidation and retaliation).”
In addition, Keith notes that “[s]eparately, the final rule eliminates explicit nondiscrimination protections for LGBT people in 10 unrelated HHS regulations, such as nondiscrimination standards for qualified health plans and the marketplaces.”
In short, as summarized in a statement by the National Health Law Program (NHeLP), “[a]fter years of executive orders and unrelenting sabotage undermining the landmark Affordable Care Act, the Trump administration has moved to officially rollback the vital regulations implementing ACA’s nondiscrimination protections for people historically discriminated against in our health care system.”
Supreme Court Decision
Days after the 1557 final rule was issued, interpreting “on the basis sex” to exclude protections for LGBTQ individuals, the U.S. Supreme Court issued a decision in Bostock v. Clayton County, Georgia (June 15, 2020, by a 6-3 majority). The Bostock decision holds that discrimination “because of sex” under Title VII of the Civil Rights Act includes, and prohibits, workplace discrimination based on sexual orientation and gender identity.
In a statement by the Human Rights Campaign (HRC) declaring that the Court “is on the right side of history for LGBTQ rights,” HRC’s President stated “This is a landmark victory for LGBTQ equality […] No one should be denied a job or fired simply because of who they are or whom they love. For the past two decades, federal courts have determined that discrimination on the basis of LGBTQ status is unlawful discrimination under federal law. Today’s historic ruling by the Supreme Court affirms that view, but there is still work left to be done.”
The Center for Medicare Advocacy strongly supports the outcome in Bostock and recognizes that it is an important step in the effort to foster equality and inclusion in our society.
What Does the Supreme Court Decision Mean for the Section 1557 Rule?
As the dust settles on these two pronouncements – one expanding the rights of the LGBTQ community and one constricting such rights (and those of other groups often discriminated against), legal analysts are assessing what the former means for the latter. There is now an obvious conflict between the Administration’s definition of sex discrimination and the Supreme Court’s definition. The Supreme Court’s definition should prevail.
As noted by Katie Keith in another Health Affairs blog post addressing this question:
From here, OCR could withdraw its rule or try to clarify its interpretation of sex nondiscrimination. Or OCR might choose to defend its interpretation in court in an inevitable legal challenge. Defending the rule would likely be an uphill battle given the Court’s resounding decision on Title VII and the fact that courts often look to Title VII when interpreting Title IX of the Education Amendment Act of 1972 (Title IX) (the basis for protection under Section 1557).
Echoing that courts have consistently looked to Title VII to construe Title IX, University of Texas law professor Liz Sepper posits that the Administration’s attempt to roll back 1557’s protections “as to LGBTQ discrimination” is “dead in the water” (see her analysis on Twitter here). Sepper notes that Bostock won’t remedy the many “bad interpretations that narrow antidiscrimination law – for now, it won’t apply to health insurers the way the 2016 rule did – in ways that hurt all people – but especially transgender people.” She also notes that DHHS “put in place a religious exemption that allows many entities inclined to discriminate to continue to do so. Many fights will take place on this ground.”
Ian Millhiser writes in Vox that the reach of Bostock likely extends beyond employment discrimination, but also likely falls short of dismantling discriminatory practices implemented in the military. He notes that the decision “strongly suggests that neither educational institutions nor health care providers may discriminate against LGBTQ individuals. If that’s the case, the Trump administration’s new health care regulation should fall […]. Outside of the military […] Bostock is a sweeping decision with implications stretching far beyond employment discrimination. Though the Trans military ban may survive, much of the rest of the Trump administration’s anti-LGBTQ agenda is in serious trouble after Bostock.”
As legal battles are waged about the scope of the Bostock decision, the fate of the final 1557 Rule is unclear. Thankfully, however, it appears to be in significant jeopardy, at least with respect to discrimination against LGBTQ persons. The Center for Medicare Advocacy will continue fight to strengthen critical non-discrimination protections in health care, and beyond.
– top –
COVID-19: An Advocates Guide to Beneficiary Related Medicare Changes – Updated June 16, 2020
The global COVID-19 crisis has led to many changes in health care rules, including in the Medicare program. Most of the Medicare changes are slated to be temporary, but advocates will need to watch which provisions do and do not remain after the crisis. While a many of the changes affect health care providers, including payment and waivers of certain requirements, our Advocates Guide focuses on Medicare COVID changes that relate to beneficiaries and their access to covered care. Note: This Advocates Guide describes, but does not analyze or critique these changes.
- Read or Download the Guide at: https://www.medicareadvocacy.org/covid-19-an-advocates-guide-to-medicare-changes/
– top –
COVID-19: Advocating for Nursing Home Residents – A webinar series
Featuring Center for Medicare Advocacy Senior Policy Attorney Toby S. Edelman.
The landscape of COVID-19 response in nursing homes continues to evolve rapidly at the federal and state levels. Join the Consumer Voice, Center for Medicare Advocacy, Long Term Care Community Coalition and Justice in Aging as we review the latest updates, issuances from CMS, legislation, and strategies for advocates and families.
This series of webinars is focused on the impact of COVID-19 on long-term care facilities and their residents. Webinars scheduled for June 19, 2020 02:00 PM; June 26, 2020 02:00 PM (All times Eastern).
– top –